
Polyarteritis Nodosa (PAN)
Polyarteritis Nodosa (PAN) is a vasculitis affecting medium-sized arteries with necrotizing inflammation leading to aneurysm formation. PAN is more common in middle-aged men with a male : female ratio of 2:1.

It is associated with –
Hepatitis B virus infection (mainly)
Mononeuritis Multiplex
Renal infarcts
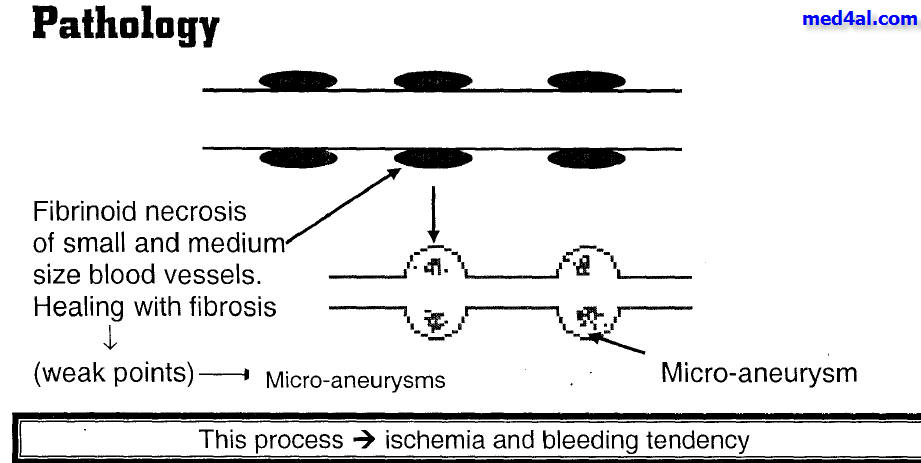
Pathology –
PAN is characterized by focal and segmental transmural necrotizing inflammation i.e. inflammation in all 4 layers of blood vessel. The exact aetiology is unknown possibly infection. As HBV is a potential trigger it could be the cause. In PAN the cell mediated immune system particularly neutrophil and macrophage get activated.
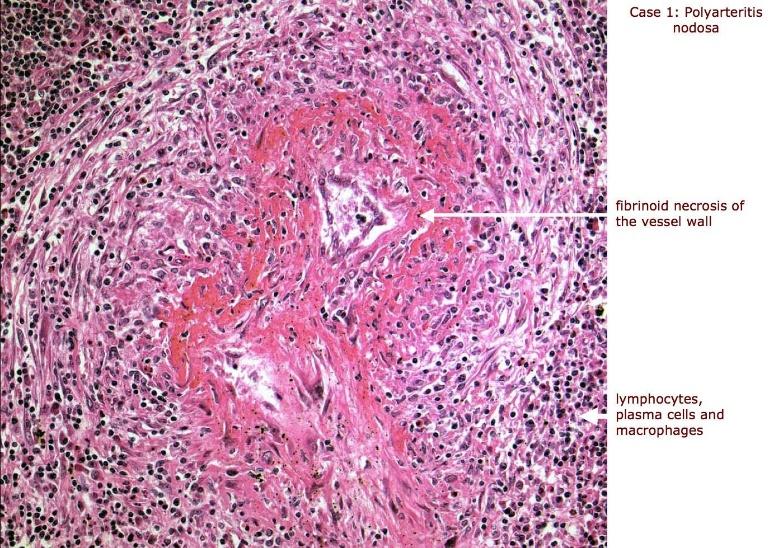
In the acute phase, neutrophil infiltrates all the layers of blood vessel and causes damage to the tissues. Then macrophage will move into that area and clean the area. Repairment of the vessel will begin. Plug formation and fibrin deposition then collagen deposition will occur. The segment of the blood vessel get fibrosed. This area is termed as fibrinoid necrosis which is a special histopathological term seen in blood vessel necrosis. Fibrinoid necrosis includes dead immune cells, collagen proteins, fibrin.
The vessels are weak and aneurysm occurs. Aneurysm is dilatation above 1 cm along the involved artery and this is characteristic for PAN. The macroscopic view of blood vessels looks like beads on a string. PAN commonly occurs in bifurcation and branching of the arteries.
Features of PAN –
In 1990, the American College of Rheumatology (ACR) established criteria for research purposes in order to differentiate PAN from other forms of vasculitis. A committee of ACR physicians selected 10 disease features of PAN; in order for PAN to be diagnosed at least 3 of the 10 ACR criteria should be present when radiographic or pathological diagnosis of vasculitis is made.
ACR criteria –
Weight loss of 4 kg or more
Livedo reticularis
Testicular pain or tenderness
Myalgia or leg weakness/tenderness
Mononeuropathy or polyneuropathy
Diastolic BP>90 mmHg
Elevated Blood urea nitrogen (BUN) or creatinine level unrelated to dehydration or obstruction
Presence of Hepatitis B surface antigen or antibody in serum
Arteriogram demonstrating aneurysm or occlusions of the visceral arteries
Biopsy of small or medium-sized artery containing polymorphonuclear neutrophils
There are some general features –
Fevers, myalgia, arthralgia, and weight loss
The most skin lesion are palpable purpura, ulceration, infarction, livedo reticularis

livedeo reticularis
PAN also involves the renal artery which can lead to renal infarction and this is due to inflammation. This leads to hypertension secondary to Renin-Angiotensin-Aldosterone System (RAAS) activation but glomerulonephritis is rare (in contrast to microscopic polyangiitis)
Mnemonic to memorize PAN
PAN LOST + Renal failure
P – Pyrexia, p-ANCA
A – Arthralgia
N – Neuropathy
L – Livedoreticularis
O – Over BP (hypertension)
S – Serology for HBV positive
T – Testicular Pain
Renal failure – oligouria, haematuria
Investigations –
Conventional or magnetic resonance angiography – confirmatory which shows multiple aneurysms and smooth narrowing of mesenteric, hepatic and renal systems

Biopsy of blood vessel, muscle and sural nerve - focal and segmental transmural necrotizing inflammation

Serology for HBV
Blood urea nitrogen and serum creatinine – increased
p-ANCA - + ve
CBC with ESR – in active disease leucocytosis, elevated ESR
Urine RME
Treatment –
High dose glucocorticoid
Immunosuppressants –
Cyclophosphamide
N.B. This drugs should never be taken without the consult of a doctor







No comments